
Nitrous Oxide and Autism
Usage of nitrous in labour should be banned.
Say NO to Nitrous
-
Vitamin B12 loading of the brain happens predominantly in the womb, with little more vitamin B12 loading of the brain for the rest of life
-
Vitamin B12 loading of the brain increases progressively as the foetus matures.
-
Vitamin B12 deficiency in the neonate is associated with delayed physical and mental development.
-
Use of Nitrous Oxide during pregnancy can result in the formation of toxic, and inactive NO-Co(III)Cobalamin
-
Reaction of Nitrous oxide with vitamin B12 is more likely in those who are functionally B12 deficient
-
The effect of Nitrous oxide is higher in children with MTHFR +/+ or MTRR +/+ polymorphisms
-
Serum levels of vitamin B12 can be normal or elevated - Paradoxical B12 deficiency
-
Children with Paradoxical B12 deficiency due to Nitrous intoxication, will not respond to MethylCo(III)B12 until there is new synthesis of methionine synthase.
-
Amounting evidence suggests that depending upon dose, mothers can also be affected by Nitrous.
-
Data suggests that even after years of supplementation with Adenosylcobalamin and methylcobalamin that it is almost impossible to displace NO-Co(III)-Cbl.
Vitamin B12 deficiency and Nitrous oxide and anaesthetics.
Methionine synthase binds to MethylCo(III)B12 which subsequently acts as a Methyl Donor to convert Homocysteine to Methionine, and the resultant Co(I)B12 can act as an acceptor for incoming methyl groups such as those on 5-methyltetrahydrofolate.
MethylCo(III)B12 + Homocysteine [Methionine Synthase] <=> Co(I)B12 + Methionine
Co(I)B12 + 5MTHF [Methionine Synthase] <=> MethylCo(III)B12 + THF
This donor/acceptor function can be dramatically reduced through exposure to Nitrous oxide either as an anaesthetic or though inhalation from a "Nang" which can then have disastrous affects on the function of vitamin B12, and its role in methylation. During the methylation reaction of
MethylCo(III)B12 + Homocysteine [Methionine Synthase], the product, Co(I)B12 + Methionine is formed. In the absence of 5MTHF, free Co(I)B12 can readily reacts with nitrous oxide to form NO-Co(III)B12, which is inactive, yet will “clog up” methylation by Methionine synthase, and irreversibly inactivate the enzyme, hence explaining the toxicity of Nitrous oxide.Co(I)B12 + Nitrous Oxide <=> NO-Co(III)B12
The NO-Co(III)cobalamin has an extremely long half-life and is resistant to loss of the NO moiety, meaning that the child may be "stuck" with it for life time. Normally, in the absence of incoming folate, Co(I)B12 is oxidized to Co(II)B12 and MethylCo(III)B12 is formed by the action of MTRR and SAM. If this does not occur, methionine synthase releases Co(II)B12 and thereby frees up the binding site for MethylCo(III)B12. The Co(II)B12 then is secreted into serum and so contributes to the elevated serum B12 levels. Unless functional B12 markers, such as MMA and homocysteine are measured it is not possible to tell if the vitamin B12 is functionally active or inactive. Hence Paradoxical B12 deficiency will result. Thus, poisoning with nitrous oxide is very different to functional B12 deficiency due to folate, or functional B2 deficiency, in that whilst Co(II)B12 or Co(I)B12 can be converted to MethylCo(III)B12, thereby restoring activity of the [MethylCo(III)B12-methionine synthase] complex, NO-Co(III)B12 cannot be displaced and thereby regenerate the activity of the enzyme.
Higher levels of Co(I)B12 are present in functional B2 deficiency, such as occurs in Iodine, Selenium and/or Molybdenum deficiency, due to lack of activity of the FAD/NADH-dependent MTHFR enzyme, particularly in those mutations in the MTHFR protein, or in those with a diet low in folate, thereby making those individuals more susceptible to the action of Nitrous oxide. The inactive NO-Co(III)B12 would be indistinguishable from inactive Co(II)B12, and when measured in the current total serum B12 and the inappropriately named active B12 tests, as they do not distinguish which analogue of cobalamin is being measured, cyanocobalamin, hydroxycobalamin, methylcobalamin, adenosylcobalamin, Co(II)cobalamin, Co(I)cobalamin, glutathionyl-Co(III)cobalamin or NO-Co(III)cobalamin, to name but a few. in indication of the extent of damage that nitrous can do to the nervous system can be gleaned from those who use Nangs, and their devastating neurological consequences. Reports of side-effects include “subacute-onset, progressive distal lower limb sensory symptoms and unsteadiness”, “subacute combined degeneration of the cord”” ataxia and progressive paresis”, depression, development of diseases of the brain, spine and nerves. The severity of these reactions has led the UK government to consider criminalizing the use of Nitrous Oxide. Genetically, Nitrous oxide sensitivity should be higher in those with MTRR +/+ mutations, as is found for the following SNPs, MTRRG12099A, MTRRA66G, and in MTHFR mutations A1298C, and rs13306571
N2O inactivates methionine synthase in everyone
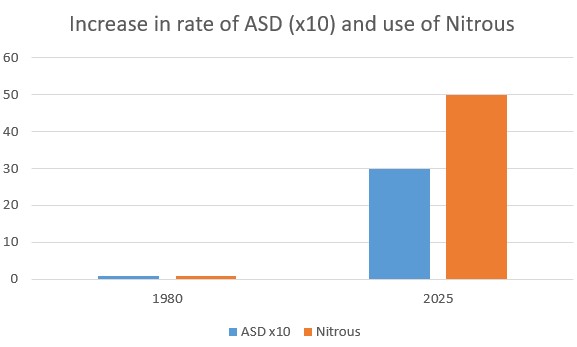
Nitrous oxide was commonly used as an anaesthetic gas, yet as long ago as 1956 (Lassen et al, 1956) it was realized that the activity of vitamin B12 was destroyed by nitrous oxide use and could cause megaloblastic anemia. In 1968, Banks and co-workers demonstrated that nitrous oxide could react with the cobalt in vitamin B12 and lead to the inactive NO-Co(III)B12 complex. The destruction of the activity of vitamin B12 is dependent upon the time and dose of administration of nitrous, with over 50% of individuals producing signs of megaloblastic depression of bone marrow function (Nunn and Chanarin, 1978). As early as 1978 (Amess et al, 1987) the use of nitrous oxide for anaesthesia was found to be contra-indicated, yet to this day it is still used, and many individuals report signs of B12 deficiency following use. Unbelievably, despite numerous publications showing poor outcomes of nitrous oxide use in pregnancy, and several demonstrating an association between nitrous and autism, and over 200 publications, demonstrating inactivation of vitamin B12 with subsequent sequelae, clinicians in the US, UK and Australia claim "“ Initiation and management of nitrous oxide by registered nurses is a safe and cost-effective option for labor pain.”. In the UK, up to 77% of patients use inhaled nitrous for labour analgesia(See PDF). One of the problems with Nitrous inactivation of vitamin B12 activity is that the levels of B12 in serum still remain high, yet paradoxically the B12 is inactive - as per the discussion on paradoxical vitamin B12 deficiency. Unbelievably, nitrous oxide is still used as an anaesthetic to this day in the USA ,UK and Australia, both on mothers during pregnancy, and also on young children. Evidence suggests that this alone is responsible for many cases of autism (Xin et al, 2024). It has been known for over 40 years that the use of nitrous oxide in anaesthesia (laughing gas) or in recreational abuse, can cause vitamin B12 deficiency (Shah and Murphy, 2019: Tani etal, 2019; Oussalah etal, 2019; Chi, 2018; Stockton etal, 2017; Massey etal, 2016: Garakani etal, 2014; Safari etal, 2013; Chiang etal, 2013; Krajewski etal, 2007; Cohen etal, 2007; Jameson etal, 1999; Smith, 2001: Deleu etal, 2001; Mayall, 1999; Horne and Holloway, 1997: Kinsella and Green 1995; Carmel etal, 1993; Koblin etal,1990; O'Leary etal, 1985; van der Westhuyzen and Metz, 1984; 1982; Lumb etal, 1982; Kondo etal, 1981: Seteinberg etal, 1981; McKenna etal, 1980; Linnell etal, 1978; Deacon etal, 1978). Post surgical complications of the use of Nitrous include peripheral neuropathy (Neuveu etal, 2019: Egan, 2018: Kaski etal, 2017; Richardson 2010), metabolic encephalopathy (Vive etal, 2019), myeloneuropathy (Edigin etal, 2019; Friedlander and Davies, 2018; Alt etal, 2011; Waklawik etal, 2003; Sesso etal, 1999: Nestor and Stark, 1996), neuropathy (Gullestrup etal, 2019; Conaerts etal, 2017:Middleton and Roffers, 2018), pancytopenia (Norris and Mallia, 2019), Myopathy (Williamson etal, 2019), myelopathy (Dong etal, 2019; Mancke etal, 2016; Probasco etal, 2011: Hathout and El-Saden, 2011; Pema et al, 1998), severe neuropsychiatric symptoms (Lundin etal, 2019), combined degeneration of the spinal chord (Lan etal, 2019; Patel etal, 2018; Anderson etal, 2018; Antonucci, 2018; Keddie etal, 2018; El-sadawi etal, 2018; Yuan etal 2017: Buizert etal, 2017; Chen and Huang, 2016; Pugliese etal, 2015: Chaugny etal, 2014; Cheng etal, 2013; Lin etal, 2011; Wijesekera, etal, 2009; Renaud etal, 2009: Wu etal, 2007; Ahn and Brown, 2005 Ilniczky etal, 2003: Beltramello etal, 1998: Rosener and DIchgans, 1996), neurotoxicity (Johnsonn etal, 2018), neuronopathy (Morris etal, 2015), polyneuropathy (Alarcia etal, 1999), psychosis (Sethi et, al, 2006), dementia (El Otmani etal, 2007), ataxia (Miller etal, 2004), megaloblastic anemia (Barbosa etal, 2000), neurological impairment (McNeeely etal, 2000), neurologic decompensation (Felmet etal, 2000), neurologic degeneration (Flippo and Holder, 1993), spastic paraparesis (Lee etal, 1999). Curiously, Nitrous is still recommended by the American Association of Anesthesiologists, NSW Department of Health, and the Association of Anesthesiologists, the New Zealand College of Midwives.. In fact, several countries with high standards of healthcare, such as Canada, Sweden, Australia, Finland, and the United Kingdom, use a blend of 50% oxygen and 50% nitrous oxide to treat pain during labour. Whilst they do not express concerns about potential damage to the newborn, they do, however, express concerns about the potential effect on Global warming, which is of greater concern than the effect on the neonatal brain!! The rational appears to be due to the replacement of epidural medication, with its risk on the spine, with the nitrous oxide. This attitude typifies the medical profession, treat the problem now, worry about the side effects later. We have contacted numerous hospitals, the Royal Children's Hospital Melbourne, Mayo Clinic Kopabirth, NZ College of Midwives, midwife associations, The America Pregnancy Association, Queensland Government, The Royal Australian and New Zealand College of Gynecology ("Excellence in women's health"), Doctors for the Environment and anaesthesiologists expressing our concerns yet not one has "returned our call". Atrocious!! Interestingly, the increase in the use of Nitrous from around 1% of births in 1980, in 2011-2014 when it is was 12% to 35=55% of births in 2024, has paralleled the rise in the rate of autism from <0.1% to now ~ 3%. In response to concerns about health, Dr Vitoria Eley of Queensland Department of Health "Great to see you engaging with the anaesthesia literature"..Queensland Government "Nitrous Oxide : Gas is safe for your baby..." Estimates suggest that if a woman chooses nitrous oxide, she has an 8-10% chance of having a baby who subsequently is diagnosed with autism, and a 25% chance of the child having ADHD or OCD. Use of Nitrous is so frequent that hospitals are using scrubbers to try to remove this greenhouse gas (Khan-Perez et al, 2022). Despite the well known dangers of Nitrous, institutions such as RANZCOG are still recommending the use of Nitrous to pregnant women. The American College of Obstetricians and Gynecologists have Diregarded all the publications on the dangers and nitrous and have take the view that have decided that since there are no studies on the use of Nitrous and the neonate, that they will disregard the literature and instead of erring on the side of caution have dispelled the possibility of harm (Home | ACOG)
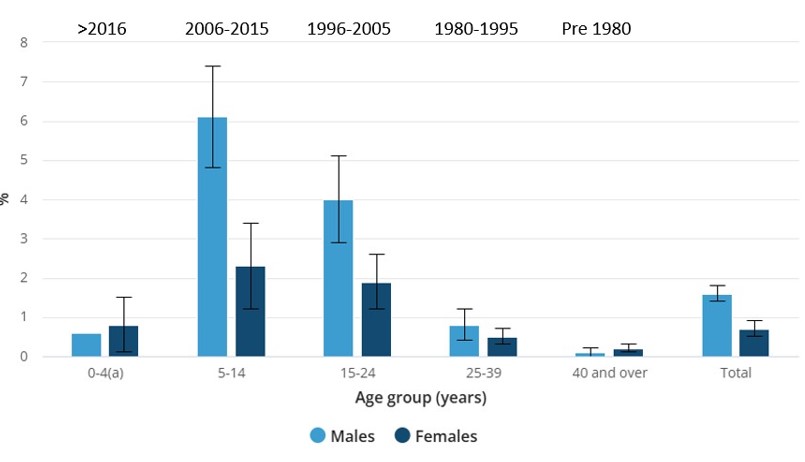
When one examines the age ranges for both ASD and for AD, it is clear that there is some event that occurred, or some change that has occurred, since 1980, that has started the dramatic increase in the rate of autism. All of the children that we have data for who have ASD or ADHD, are functionally deficient in vitamin B12, with normal to elevated serum vitamin B12, and standard markers MMA, HVA, VMA, QA, KA, 5HIAA, pyroglutamic acid and phosphoric acid.
N2O inhibition of methionine synthase is rapid, potent, and irreversible patients in all , and harmful in a substantial proportion of patients that are not identified before exposure
There are several groups who have shown the deleterious effects of nitrous on the brain. Thus Selzer (2003) demonstrated increased susceptibly of those with MTHFR mutations to Nitrous Oxide, with a report of death in a child exposed to nitrous on two separate occasions (Selzer 2003) and Kalikiri and co-workers (2004) found a dramatic change in MMA and homocysteine levels in nitrous, as too Baum (2007). The study findings of a mechanistic link between nitric oxide levels and autism spectrum disorder are significant (Jackson, 2023).
The extent of damage to the brain will be dependent upon how long the child was exposed to nitrous oxide, and at what stage their development was at. Hence areas of the brain that were most active at the time of exposure are most likely to be affected the most. At time of birth this would be cerebellum, followed after birth by the subcortical areas and then the cerebral cortex. Of note, Human fetal/neonatal and geriatric kinetics of inactivation and reactivation are unknown in any tissue. N2O inhibition of methionine synthase is rapid, potent, and irreversible patients in all, and harmful in a substantial proportion of patients that are not identified before exposure
N2O is the only inhaled anesthetic that will kill everyone who breathes it at clinical concentrations for 5-7 day
Identification
of Nitrous oxide intoxicationDevelopmental delay, due to nitrous oxide intoxication is not detectable for months after the birth. Hence, statements, such "As does not harm the baby" have little to no verification. Whilst there is a scintilla of evidence about brain damage with nitrous oxide it would not be prudent to continue the practise, particularly since the association of increased use of nitrous parallels the increased rate of autism.
Deleterious consequences of nitrous are long-lasting, not “short acting”
Symptoms include Complete Regression into autism, tT
he loss of developmental skills such as: Expressive and receptive language, Gross motor skills, Fine motor skills, reduced Cognitive skills, Overall neurological deterioration (skill loss may be permanent in some children)Nitrous oxide intoxication and the mother
Evidence is mounting that whilst the mother may not show signs of nitrous intoxication at the time of birth, many show evidence of vitamin B12 deficiency later, with serum levels of vitamin B12 being raised.
Treatment of Nitrous oxide intoxication
Treatment of Nitrous oxide inhalation is possible if it is done early, however, treatment has to be quick, or permanent damage is done. Successful treatment, though appears to occur mainly in those who had an absolute B12 deficiency,. Hence if the body normally has 300-350 pmol/ml transcobalamin-bound vitamin B12, but in deficiency it has less than 200 pmol/ml, then administering excess vitamin B12 will cause a reduced but functional sufficiency of vitamin B12. These people can be "rescued" by the addition of high doses of vitamin B12, incoming B12 will still show a response. However, in individuals with a saturated transport system and a deficiency in functional B2, and particularly in those with MTHFR and MTRR mutations, nitrous intoxication will affect all the B12, and so addition of excess B12 will not be effective. This has been noted by various workers, who have claimed some success in treatment of some of the individuals who had nitrous, but not all (Brunt et al, 2024; Boulin et al, 2025; Einsiedler et al, 2022; Zheng et al, 2020; Xiang et al, 2021) This, though, is not what happens following exposure during labour, and so the potential for treatment is lost, particularly given that diagnosis of neurological damage is not done until many months or even years later. There is hope though, but it depends upon making sure that you get any deficiencies such as functional B2 and B12 deficiencies right first, and then slowly let nature take its course. In those who are severely affected this may take years!!
Say NO to the use of Nitrous.
Markers of functional B12 deficiency due to
Nitrous oxide intoxicationMarkers of functional B12 deficiency would be very similar to those observed with with functional B2/B12 deficiency, and would include
-
Elevated or normal serum vitamin B12
-
Elevated MMA and homocysteine
-
Elevated neurotransmitter metabolites, HVA, VMA, QA, KA, 5HIAA
-
Elevated pyroglutamic acid
-
Reduced SAM:SAH ratio
-
Reduced GSH:GSSG ratio
-
Low serum creatinine
-
Lack of correlation between MMA and markers of Methyl B12 deficiency.
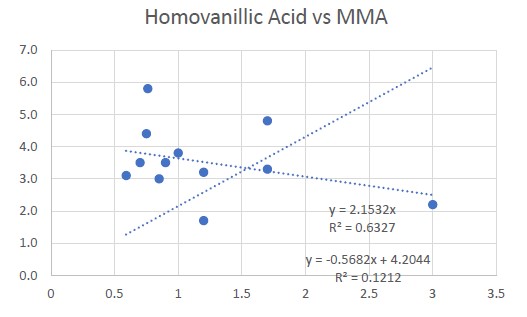
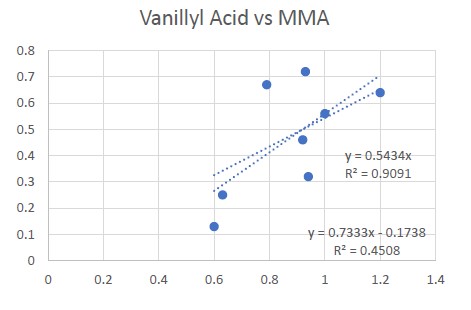
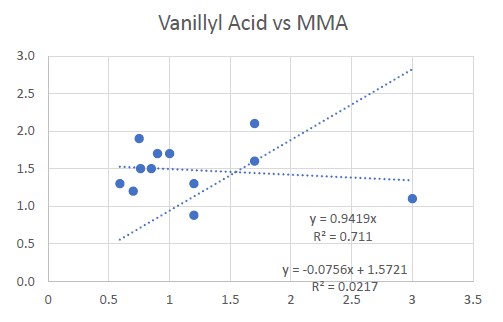
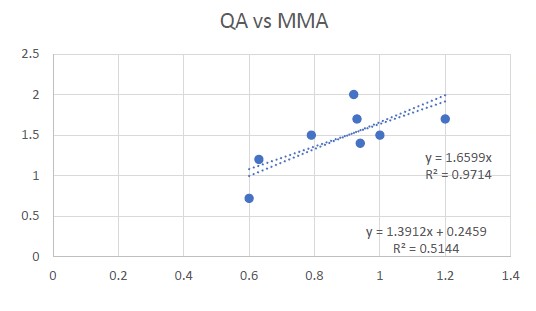
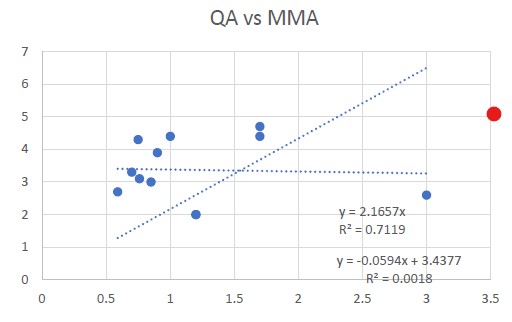
Comparison of Methyl deficiency markers against MMA.
Neurotypical (left) vs ASD (right)
Comparison of MMA vs the methyl B12 deficiency markers HVA, VMA and QA in normal individuals reveals a close linear correlation. In comparison there was little correlation between HVA, VMA and QA and MMA in the ASD example. Data was collected over a 4 year period of treatment with Adenosyl/Methyl B12. In that period MMA levels decreased in both groups, and methyl deficiency markers reduced in the control, however, there was no evidence of change of Methyl B12 deficiency markers in the ASD individual.
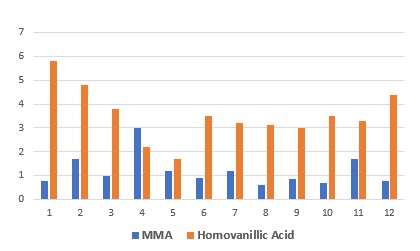
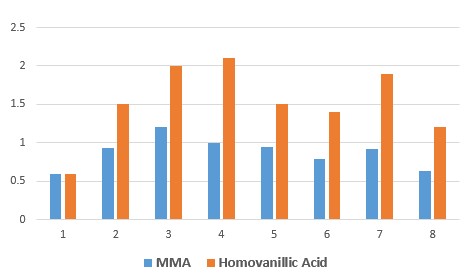
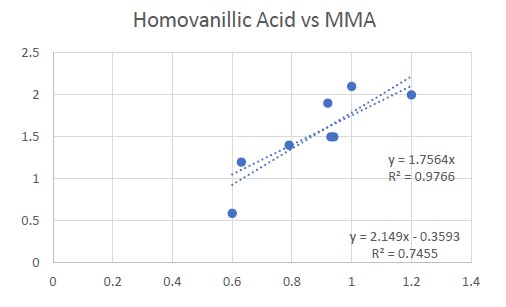
Comparison of HVA to MMA between Nitrous affected autism child and B12 deficient neurotypical individaul shows a considerable difference in the ratio of HVA:MMA. Hence, in the NT indivdual, HVA generally has a close relationship to MMA, with 2:1 being the highest ratio, , but in the nitrous oxide exposed child, the ratio of HVA:MMA varies considerable from 5:1 to 1.3: 1 with many data points >3:1. In addition, despite MMA being less than 1.0, in the nitrou affected child HVA has persisted above 3.0. In contrast the NT individual HVA was below 2.0 for most oft he data, and reached 1.2.
The data is commensurate with what is known about nitrous poisoning in babies. Hence, " babies affected by nitrous have a life long mental and often physical disability, requiring constant care, and repetitive medical and educational costs, often costing over $50,000 per year".
Effect of Nitrous on the brain
Nitrous mainly affects areas of the brain involved in neurotransmission, sensory processing and cognitive function. Exposure to nitrous during delivery affects those areas under-rapid development and synaptic formation. Areas to be affected would be the Frontal Cortex, which affects executive functioning and decision making. Nitrous acts as an NMDA receptor antagonist and affects glutamatergic signaling, affecting attention, impulse control and higher cognitive functions. Nitrous affects dopaminergic functioning thereby causing movement disorders, and difficulties in co-ordination. Nitrous also affects the cerebellum, potentially affecting motor development and causing difficulties with balance. Nitrous also has been linked to subacute spinal degeneration, thereby resulting in neuropathy, weakness and altered reflexes.
Usage of nitrous in labour should be totally banned.
Thalidomide similarities
In many ways the Nitrous "story" is similar to the Thalidomide story. Hence the drug was tested on women who were not pregnant, and was found to be safe. However, when it was administered as as a sedative and a treatment for morning sickness, with disastrous consequences. Potentially, though Nitrous is worse. Hence many of the thalidomide babies had limb deformities, they were otherwise OK. In contrast, babies that are affected by nitrous have a life long mental and often physical disability, requiring constant care, and repetitive medical and educational costs, often costing over $50,000 per annum.
Prevention of Nitrous oxide intoxication
Obviously prevention involves total avoidance of nitrous oxide during pregnancy. Despite the dangers of nitrous oxide, Anaesthetic Societies around the world have ignored the warnings.
In what is arguably one of the best examples of cognitive dissonance, the Anaesthetic Society of Australia has Not only failed to acknowledge the plethora of references describing the inactivation of the essential enzyme, methionine synthase by nitrous oxide, as well as the categorization of nitrous oxide as a Schedule 6 toxin, and the more recent publications on the linkage of the use of nitrous oxide to the subsequent development of autism in the babies born to mothers treated with nitrous oxide during labour, and the recent death of a young child by nitrous oxide intoxication, and the multitude of examples of degeneration of the spine in recreational nitrous oxide users, rather it has failed to modify its practise of using nitrous oxide by proclaiming that it will continue to use nitrous oxide until a clinical trial demonstrates that it harms the foetus during delivery.This "no mia culpa" attitude flies in the face of the Hippocratic oath, and more specifically ignores two of the major tenets of the oath (i) Non-maleficence, the avoidance of causing harm to patients, and (2) Prohibition of certain acts, which forbids administering poison... Hence administration of a Schedule 6 toxin to a minor (the foetus), subsequently resulting in brain damage and developmental delay of the soon to be born child.
Treatment
of Nitrous oxide intoxicationTreatment of nitrous oxide intoxication should begin as soon as possible by injection of large amounts of Methyl B12. If treatment is delayed, the RnB protocol (https://b12oils.com/rnbautism.htm ) should be used to ensure correction of functional B2 deficiency, and also high dose Adenosyl/Methyl B12, in the hope that the toxic NO-Co(III)B12 can be displaced. The longer the nitrous exposure and the longer the time until treatment is commenced, the less success there will be. For this reason, Prevention is Better than cure.
Usage of nitrous in labour should be totally banned.
Supply of a Toxic Substance to a Minor
Since October 2022 in Australia, nitrous oxide has been classified as a Schedule 6 poison, prohibited from supply to anyone under 16 due to its neurotoxic potential. Yet in obstetric practice, the same substance is administered in 50% concentration to pregnant women, resulting in involuntary fetal exposure at levels vastly exceeding occupational safety limits. The fetus — a minor under 16, unable to consent, and receiving no therapeutic benefit — is exposed to a Schedule 6 toxin at the moment of peak neurodevelopmental vulnerability. This appears inconsistent with both the intent and the letter of the Schedule 6 protections
Further to this, the clinician or associated health care worker, due to their actions in supplying a Schedule 6 poison to a person under 16 would be legally liable for any damage that this incurs.
Nitrous oxide, No Laughing Matter.
During labour, the delivery of Nitrous oxide, occurs through an exquisitely maintained Pharmaceutical window with the mother carefully ensuring that levels of nitrous never drop below the minimum effective concentration of this Schedule 6 toxin. By comparison, the Pharmaceutical Industry has yet to design such a perfect delivery system as that of the mother receiving nitrous from her health professional.
With every breath she takes, she ensures that she continuously bathes the brain of her foetus in the highly toxic, Schedule 6 toxin, nitrous oxide (One should be aware that it is illegal to give a Schedule 6 toxin to persons under the age of 16. Such a person would be the foetus, within the mother’s womb). Her search for pain relief means that the nitrous is continuously delivered at a concentration above the minimum toxic range, in an optimal delivery device, the mother. Unknowingly, the mother repeatedly breathes in a soothing gas containing 500,000 ppm of nitrous oxide, a mixture that is 20,000 times the safe upper environmental exposure limit, and delivers the nitrous, via the placenta to the soon to be delivered foetus.
The brain of the foetus, though, is not the brain of the mother. In contrast to the mother’s highly developed brain, for the foetal brain, it is the start of its neurodevelopmental journey. During the 3rd trimester of pregnancy, it is primed for its peak of differentiation and synaptogenesis. With every breath of euphoria generating feeling of the mother, more and more damage is being inflicted on the foetal brain, ensuring that it becomes progressively less capable of developing normally and so ensures that if its development does proceed, it will be greatly delayed.
In a scene akin to some gruesome horror movie, the mother repeatedly inhales mind-altering drugs in some attempt to alleviate the pain of childbirth, and with every breath, unknowingly, ensures the gradual destruction of the future cognitive and developmental capabilities of her soon to be born child.
Meanwhile, trapped within in the womb, continually flooded with toxic nitrous oxide, the foetus cannot speak up to halt the intoxication, and for many, they never will be able to speak. Whilst it is highly unlikely that any mother would deliberately bathe the brain of her unborn child in toxic levels of a Schedule 6 toxin, this has effectively and irreversibly been what she has done.
Little wonder, that some two to three years later, when her child fails to achieve its milestones and potential in life, she will not know or realize that she, and that she alone, is the reason for the child’s failure to develop. Something that will haunt her for the rest of her life.
At that time, the people who advised her that nitrous oxide was perfectly safe for her and her unborn child will be long gone and will be adopting a “no mia culpa” attitude, denying any culpability for the regressed child.
Little did she know, that the advice from those doctors, nurses and mid-wives, at the very time when she should have been able to depend upon them, and whom she trusted implicitly, was incorrect. Little did she know, that one decision on that day would completely change her life from one of joy and amazement and love of her child, to one of constant care, heartbreak, frustration and depression. A life, in which many times she will consider giving up her child to care by someone else, and in some instances even cause her and her family to commit murder and suicide. No, Nitrous is definitely no laughing matter, and should be avoided at all costs during those final hours of the foetus’ life, a life that was until that moment completely under her control.
Copyright.
The descriptions and findings on vitamin B12 and autism, is the property of B12 Oils Pty Ltd. Reproduction in whole or in part constitutes an infringement in the Copyright law. Copyright infringement carries serious penalties.
References
Nitrous Oxide and Vitamin B12 deficiency
Neveu J, Perelman S, Suisse G, Monpoux F. Severe hyperhomocysteinemia and peripheral neuropathy as side effects of nitrous oxide in two patients with
sickle cell disease. Arch Pediatr. 2019 Oct;26(7):419-421. doi: 10.1016/j.arcped.2019.09.006. Epub 2019 Oct 17. PubMed PMID: 31630905.
Edigin E, Ajiboye O, Nathani A. Nitrous Oxide-induced B12 Deficiency Presenting With Myeloneuropathy. Cureus. 2019 Aug 6;11(8):e5331. doi:10.7759/cureus.5331. PubMed PMID: 31598438; PubMed Central PMCID: PMC6777927.
Tani J, Weng HY, Chen HJ, Chang TS, Sung JY, Lin CS. Elucidating Unique Axonal Dysfunction Between Nitrous Oxide Abuse and Vitamin B12 Deficiency. Front Neurol. 2019 Jul 9;10:704. doi: 10.3389/fneur.2019.00704. eCollection 2019. PubMed PMID: 31354607; PubMed Central PMCID: PMC6633399.
Nouri A, Patel K, Montejo J, Nasser R, Gimbel DA, Sciubba DM, Cheng JS. The Role of Vitamin B(12) in the Management and Optimization of Treatment in Patients With Degenerative Cervical Myelopathy. Global Spine J. 2019 May;9(3):331-337. doi: 10.1177/2192568218758633. Epub 2018 May 17. Review. PubMed PMID: 31192102; PubMed Central PMCID: PMC6542160.
Gullestrup A, Jensen RB, Břgevig S, Nilsson PM. [Acute neuropathy and liver injury following the abuse of nitrous oxide]. Ugeskr Laeger. 2019 May 13;181(20).
pii: V12180890. Danish. PubMed PMID: 31124452.
Norris F, Mallia P. Lesson of the month 2: A case of nitrous oxide-induced pancytopenia. Clin Med (Lond). 2019 Mar;19(2):129-130. doi: 10.7861/clinmedicine.19-2-129. PubMed PMID: 30872294; PubMed Central PMCID:
PMC6454366.
Williamson J, Huda S, Damodaran D. Nitrous oxide myelopathy with functional vitamin B (12) deficiency. BMJ Case Rep. 2019 Feb 13;12(2). pii: e227439. doi:
10.1136/bcr-2018-227439. PubMed PMID: 30765444.
Lundin MS, Cherian J, Andrew MN, Tikaria R. One month of nitrous oxide abuse causing acute vitamin B (12) deficiency with severe neuropsychiatric symptoms.
BMJ Case Rep. 2019 Feb 7;12(2). pii: bcr-2018-228001. doi: 10.1136/bcr-2018-228001. PubMed PMID: 30737329.
Lan SY, Kuo CY, Chou CC, Kong SS, Hung PC, Tsai HY, Chen YC, Lin JJ, Chou IJ, Lin KL; PCHAN Study Group. Recreational nitrous oxide abuse related subacute combined degeneration of the spinal cord in adolescents - A case series and literature review. Brain Dev. 2019 May;41(5):428-435. doi: 10.1016/j.braindev.2018.12.003. Epub 2019 Jan 2. Review. PubMed PMID: 30611595.
Dong X, Ba F, Wang R, Zheng D. Imaging appearance of myelopathy secondary to nitrous oxide abuse: a case report and review of the literature. Int J Neurosci.
2019 Mar;129(3):225-229. doi: 10.1080/00207454.2018.1526801. Epub 2018 Dec 4.Review. PubMed PMID: 30234413.
Patel KK, Mejia Munne JC, Gunness VRN, Hersey D, Alshafai N, Sciubba D, Nasser R, Gimbel D, Cheng J, Nouri A. Subacute combined degeneration of the
spinal cord following nitrous oxide anesthesia: A systematic review of cases. Clin Neurol Neurosurg. 2018 Oct;173:163-168. doi: 10.1016/j.clineuro.2018.08.016.
Epub 2018 Aug 9. Erratum in: Clin Neurol Neurosurg. 2019 Feb;177:123-124. Abstract corrected. PubMed PMID: 30144777.
Jolobe OMP. Other aspects of nitrous oxide-related neuromyelopathy. Am J Emerg Med. 2019 Feb;37(2):350-351. doi: 10.1016/j.ajem.2018.05.076. Epub 2018 May 30. PubMed PMID: 29866413.
Egan W, Steinberg E, Rose J. Vitamin B(12) deficiency-induced neuropathy secondary to prolonged recreational use of nitrous oxide. Am J Emerg Med. 2018
Sep;36(9):1717.e1-1717.e2. doi: 10.1016/j.ajem.2018.05.029. Epub 2018 May 24. PubMed PMID: 29859645.
Anderson D, Beecher G, van Dijk R, Hussain M, Siddiqi Z, Ba F. Subacute Combined Degeneration from Nitrous Oxide Abuse in a Patient with Pernicious
Anemia. Can J Neurol Sci. 2018 May;45(3):334-335. doi: 10.1017/cjn.2018.15. PubMed PMID: 29756593.
Antonucci MU. Subacute Combined Degeneration from Recreational Nitrous Oxide Inhalation. J Emerg Med. 2018 May;54(5):e105-e107. doi: 10.1016/j.jemermed.2018.01.045. Epub 2018 Mar 27. PubMed PMID: 29602528.
Keddie S, Adams A, Kelso ARC, Turner B, Schmierer K, Gnanapavan S, Malaspina A, Giovannoni G, Basnett I, Noyce AJ. No laughing matter: subacute degeneration of the spinal cord due to nitrous oxide inhalation. J Neurol. 2018 May;265(5):1089-1095. doi: 10.1007/s00415-018-8801-3. Epub 2018 Mar 3. PubMed
PMID: 29502317; PubMed Central PMCID: PMC5937900.
Johnson K, Mikhail P, Kim MG, Bosco A, Huynh W. Recreational nitrous oxide-associated neurotoxicity. J Neurol Neurosurg Psychiatry. 2018 Aug;89(8):897-898. doi: 10.1136/jnnp-2017-317768. Epub 2018 Jan 24. PubMed PMID: 29367261.
Al-Sadawi M, Claris H, Archie C, Jayarangaiah A, Oluya M, McFarlane SI. Inhaled Nitrous Oxide 'Whip-Its!' Causing Subacute Combined Degeneration of
Spinal Cord. Am J Med Case Rep. 2018;6(12):237-240. doi: 10.12691/ajmcr-6-12-3. Epub 2018 Dec 26. PubMed PMID: 31058215; PubMed Central PMCID: PMC6499494.
Friedlander G, Davies T. The Last Laugh - Reversible myeloneuropathy induced by chronic nitrous oxide use. Acute Med. 2018;17(4):232-235. PubMed PMID:
30882108.
Yuan JL, Wang SK, Jiang T, Hu WL. Nitrous oxide induced subacute combined degeneration with longitudinally extensive myelopathy with inverted V-sign on
spinal MRI: a case report and literature review. BMC Neurol. 2017 Dec 28;17(1):222. doi: 10.1186/s12883-017-0990-3. PubMed PMID: 29282001; PubMed
Central PMCID: PMC5745895.
Conjaerts SHP, Bruijnes JE, Beerhorst K, Beekman R. [Nitrous oxide-induced polyneuropathy]. Ned Tijdschr Geneeskd. 2017;161:D2044. Dutch. PubMed PMID:
29192578.
Kaski D, Kumar P, Murphy E, Warner TT. Iatrogenic B12-deficient peripheral neuropathy following nitrous oxide administration for functional tonic leg spasm:
A case report. Clin Neurol Neurosurg. 2017 Sep;160:108-110. doi:10.1016/j.clineuro.2017.07.006. Epub 2017 Jul 6. PubMed PMID: 28709008.
Stockton L, Simonsen C, Seago S. Nitrous oxide-induced vitamin B12 deficiency. Proc (Bayl Univ Med Cent). 2017 Apr;30(2):171-172. PubMed PMID: 28405070; PubMed Central PMCID: PMC5349816.
Buizert A, Sharma R, Koppen H. When the Laughing Stops: Subacute Combined Spinal Cord Degeneration Caused by Laughing Gas Use. J Addict Med. 2017
May/Jun;11(3):235-236. doi: 10.1097/ADM.0000000000000295. PubMed PMID: 28166085.
40: Chen HJ, Huang CS. Nitrous Oxide-induced Subacute Combined Degeneration Presenting with Dystonia and Pseudoathetosis: A Case Report. Acta Neurol Taiwan. 2016 Jun 15;25(2):50-55. PubMed PMID: 27854092.
Mancke F, Kaklauskaitė G, Kollmer J, Weiler M. Psychiatric comorbidities in a young man with subacute myelopathy induced by abusive nitrous oxide consumption: a case report. Subst Abuse Rehabil. 2016 Sep 29;7:155-159. eCollection 2016.PubMed PMID: 27729826; PubMed Central PMCID: PMC5047713.
Massey TH, Pickersgill TT, J Peall K. Nitrous oxide misuse and vitamin B12 deficiency. BMJ Case Rep. 2016 May 31;2016. pii: bcr2016215728. doi:10.1136/bcr-2016-215728. PubMed PMID: 27247211; PubMed Central PMCID: PMC4904416.
Duque MA, Kresak JL, Falchook A, Harris NS. Nitrous Oxide Abuse and Vitamin B12 Action in a 20-Year-Old Woman: A Case Report. Lab Med. 2015 Fall;46(4):312-5. doi: 10.1309/LM0L9HAVXCHF1UQM. PubMed PMID: 26489675.
Pugliese RS, Slagle EJ, Oettinger GR, Neuburger KJ, Ambrose TM. Subacute combined degeneration of the spinal cord in a patient abusing nitrous oxide and
self-medicating with cyanocobalamin. Am J Health Syst Pharm. 2015 Jun 1;72(11):952-7. doi: 10.2146/ajhp140583. PubMed PMID: 25987690.
Morris N, Lynch K, Greenberg SA. Severe motor neuropathy or neuronopathy due to nitrous oxide toxicity after correction of vitamin B12 deficiency. Muscle
Nerve. 2015 Apr;51(4):614-6. doi: 10.1002/mus.24482. Epub 2015 Feb 24. PubMedPMID: 25297001.
Garakani A, Welch AK, Jaffe RJ, Protin CA, McDowell DM. Psychosis and low cyanocobalamin in a patient abusing nitrous oxide and cannabis. Psychosomatics.
2014 Nov-Dec;55(6):715-9. doi: 10.1016/j.psym.2013.11.001. Epub 2013 Nov 5.PubMed PMID: 24367897.
Safari A, Emadi F, Jamali E, Borhani-Haghighi A. Clinical and MRI manifestations of nitrous oxide induced vitamin B12 deficiency: A case report. Iran J Neurol. 2013;12(3):111-3. PubMed PMID: 24250916; PubMed Central PMCID: PMC3829298.
Chiang TT, Hung CT, Wang WM, Lee JT, Yang FC. Recreational nitrous oxide abuse-induced vitamin B12 deficiency in a patient presenting with
hyperpigmentation of the skin. Case Rep Dermatol. 2013 Jun 29;5(2):186-91. doi: 10.1159/000353623. Print 2013 May. PubMed PMID: 23898268; PubMed Central PMCID: PMC3724136.
Chaugny C, Simon J, Collin-Masson H, De Beauchęne M, Cabral D, Fagniez O, Veyssier-Belot C. [Vitamin B12 deficiency due to nitrous oxide use: unrecognized
cause of combined spinal cord degeneration]. Rev Med Interne. 2014 May;35(5):328-32. doi: 10.1016/j.revmed.2013.04.018. Epub 2013 Jun 14. French. PubMed PMID: 23773901.
Cheng HM, Park JH, Hernstadt D. Subacute combined degeneration of the spinal cord following recreational nitrous oxide use. BMJ Case Rep. 2013 Mar 8;2013.
pii: bcr2012008509. doi: 10.1136/bcr-2012-008509. PubMed PMID: 23476009; PubMed Central PMCID: PMC3618752.
Ghobrial GM, Dalyai R, Flanders AE, Harrop J. Nitrous oxide myelopathy posing as spinal cord injury. J Neurosurg Spine. 2012 May;16(5):489-91. doi:10.3171/2012.2.SPINE11532. Epub 2012 Mar 2. PubMed PMID: 22385084.
Probasco JC, Felling RJ, Carson JT, Dorsey ER, Niessen TM. Teaching NeuroImages: myelopathy due to B₁₂ deficiency in long-term colchicine treatment
and nitrous oxide misuse. Neurology. 2011 Aug 30;77(9):e51. doi:10.1212/WNL.0b013e31822c910f. PubMed PMID: 21876193.
Lin RJ, Chen HF, Chang YC, Su JJ. Subacute combined degeneration caused by nitrous oxide intoxication: case reports. Acta Neurol Taiwan. 2011 Jun;20(2):129-37. Review. PubMed PMID: 21739392.
Hathout L, El-Saden S. Nitrous oxide-induced B12 deficiency myelopathy: Perspectives on the clinical biochemistry of vitamin B12. J Neurol Sci. 2011 Feb
15;301(1-2):1-8. doi: 10.1016/j.jns.2010.10.033. Epub 2010 Nov 26. Review. PubMed PMID: 21112598.
Alt RS, Morrissey RP, Gang MA, Hoffman RS, Schaumburg HH. Severe myeloneuropathy from acute high-dose nitrous oxide (N2O) abuse. J Emerg Med. 2011
Oct;41(4):378-80. doi: 10.1016/j.jemermed.2010.04.020. Epub 2010 Jun 7. PubMed PMID: 20605391.
Richardson PG. Peripheral neuropathy following nitrous oxide abuse. Emerg Med Australas. 2010 Feb;22(1):88-90. doi: 10.1111/j.1742-6723.2009.01262.x. PubMedPMID: 20152009.
Wijesekera NT, Davagnanam I, Miszkiel K. Subacute combined cord degeneration: a rare complication of nitrous oxide misuse. A case report. Neuroradiol J. 2009
May 15;22(2):194-7. Epub 2009 May 15. PubMed PMID: 24207040.
Renard D, Dutray A, Remy A, Castelnovo G, Labauge P. Subacute combined degeneration of the spinal cord caused by nitrous oxide anaesthesia. Neurol Sci.
2009 Feb;30(1):75-6. doi: 10.1007/s10072-009-0013-2. Epub 2009 Jan 24. PubMed PMID: 19169627.
Jameson M, Roberts S, Anderson NE, Thompson P. Nitrous oxide-induced vitamin B(12) deficiency. J Clin Neurosci. 1999 Mar;6(2):164-6. PubMed PMID: 18639144.
Sethi NK, Mullin P, Torgovnick J, Capasso G. Nitrous oxide "whippit" abuse presenting with cobalamin responsive psychosis. J Med Toxicol. 2006 Jun;2(2):71-4. Review. PubMed PMID: 18072118; PubMed Central PMCID: PMC3550053.
Krajewski W, Kucharska M, Pilacik B, Fobker M, Stetkiewicz J, Nofer JR, Wronska-Nofer T. Impaired vitamin B12 metabolic status in healthcare workers
occupationally exposed to nitrous oxide. Br J Anaesth. 2007 Dec;99(6):812-8. Epub 2007 Oct 20. PubMed PMID: 17951609.
Wu MS, Hsu YD, Lin JC, Chen SC, Lee JT. Spinal myoclonus in subacute combined degeneration caused by nitrous oxide intoxication. Acta Neurol Taiwan. 2007
Jun;16(2):102-5. PubMed PMID: 17685135.
Singer MA, Lazaridis C, Nations SP, Wolfe GI. Reversible nitrous oxide-induced myeloneuropathy with pernicious anemia: case report and literature review. Muscle Nerve. 2008 Jan;37(1):125-9. PubMed PMID: 17623854.
Cohen Aubart F, Sedel F, Vicart S, Lyon-Caen O, Fontaine B. [Nitric-oxide triggered neurological disorders in subjects with vitamin B12 deficiency]. Rev Neurol (Paris). 2007 Mar;163(3):362-4. French. PubMed PMID: 17404524.
Ahn SC, Brown AW. Cobalamin deficiency and subacute combined degeneration after nitrous oxide anesthesia: a case report. Arch Phys Med Rehabil. 2005 Jan;86(1):150-3. PubMed PMID: 15641006.
Miller MA, Martinez V, McCarthy R, Patel MM. Nitrous oxide "whippit" abuse presenting as clinical B12 deficiency and ataxia. Am J Emerg Med. 2004 Mar;22(2):124. PubMed PMID: 15011232.
Waclawik AJ, Luzzio CC, Juhasz-Pocsine K, Hamilton V. Myeloneuropathy from nitrous oxide abuse: unusually high methylmalonic acid and homocysteine levels.
WMJ. 2003;102(4):43-5. Erratum in: WMJ. 2003;102(6):5. PubMed PMID: 12967021.
Ilniczky S, Jelencsik I, Kenéz J, Szirmai I. MR findings in subacute combined degeneration of the spinal cord caused by nitrous oxide anaesthesia--two cases.
Eur J Neurol. 2002 Jan;9(1):101-4. PubMed PMID: 11784385.
Barbosa L, Leal I, Timóteo AT, Matias T. [Acute megaloblastic anemia caused by inhalation of nitrous oxide in a patient with multiple autoimmune pathology]. Acta Med Port. 2000 Sep-Dec;13(5-6):309-12. Portuguese. PubMed PMID: 11234497.
Deleu D, Hanssens Y, Louon A. Nitrous oxide-induced cobalamin deficiency. Arch Neurol. 2001 Jan;58(1):134-5. PubMed PMID: 11176951.
McNeely JK, Buczulinski B, Rosner DR. Severe neurological impairment in an infant after nitrous oxide anesthesia. Anesthesiology. 2000 Dec;93(6):1549-50.
PubMed PMID: 11149458.
Felmet K, Robins B, Tilford D, Hayflick SJ. Acute neurologic decompensation in an infant with cobalamin deficiency exposed to nitrous oxide. J Pediatr. 2000 Sep;137(3):427-8. PubMed PMID: 10969273.
Marié RM, Le Biez E, Busson P, Schaeffer S, Boiteau L, Dupuy B, Viader F. Nitrous oxide anesthesia-associated myelopathy. Arch Neurol. 2000 Mar;57(3):380-2. PubMed PMID: 10714665.
Göthe CJ, Petersson G. [Nitrous oxide and cobalamin deficiency]. Lakartidningen. 1999 Dec 15;96(50):5609. Swedish. PubMed PMID: 10643221.
Lindstedt G. [Nitrous oxide can cause cobalamin deficiency. Vitamin B12 is a simple and cheap remedy]. Lakartidningen. 1999 Nov 3;96(44):4801-5. Review.
Swedish. PubMed PMID: 10584542.
Alarcia R, Ara JR, Serrano M, García M, Latorre AM, Capablo JL. [Severe polyneuropathy after using nitrous oxide as an anesthetic. A preventable disease?]. Rev Neurol. 1999 Jul 1-15;29(1):36-8. Spanish. PubMed PMID: 10528308.
Sesso RM, Iunes Y, Melo AC. Myeloneuropathy following nitrous oxide anesthaesia in a patient with macrocytic anaemia. Neuroradiology. 1999 Aug;41(8):588-90. PubMed PMID: 10447571.
Mayall M. Vitamin B12 deficiency and nitrous oxide. Lancet. 1999 May 1;353(9163):1529. PubMed PMID: 10232347.
Pema PJ, Horak HA, Wyatt RH. Myelopathy caused by nitrous oxide toxicity. AJNR Am J Neuroradiol. 1998 May;19(5):894-6. PubMed PMID: 9613506.
Beltramello A, Puppini G, Cerini R, El-Dalati G, Manfredi M, Roncolato G, Idone D, De Togni L, Turazzini M. Subacute combined degeneration of the spinal
cord after nitrous oxide anaesthesia: role of magnetic resonance imaging. J Neurol Neurosurg Psychiatry. 1998 Apr;64(4):563-4. PubMed PMID: 9576560; PubMed
Central PMCID: PMC2170040.
Horne DW, Holloway RS. Compartmentation of folate metabolism in rat pancreas: nitrous oxide inactivation of methionine synthase leads to accumulation of 5-methyltetrahydrofolate in cytosol. J Nutr. 1997 Sep;127(9):1772-5. PubMed PMID: 9278558.
Takács J. [N2O-induced acute funicular myelosis in latent vitamin B 12 deficiency]. Anasthesiol Intensivmed Notfallmed Schmerzther. 1996 Oct;31(8):525-8. German. PubMed PMID: 9019188.
Nestor PJ, Stark RJ. Vitamin B12 myeloneuropathy precipitated by nitrous oxide anaesthesia. Med J Aust. 1996 Aug 5;165(3):174. PubMed PMID: 8709889.
Rösener M, Dichgans J. Severe combined degeneration of the spinal cord after nitrous oxide anaesthesia in a vegetarian. J Neurol Neurosurg Psychiatry. 1996
Mar;60(3):354. PubMed PMID: 8609528; PubMed Central PMCID: PMC1073874.
Hadzic A, Glab K, Sanborn KV, Thys DM. Severe neurologic deficit after nitrous oxide anesthesia. Anesthesiology. 1995 Oct;83(4):863-6. Review. PubMed PMID: 7574068.
King M, Coulter C, Boyle RS, Whitby RM. Neurotoxicity from overuse of nitrous oxide. Med J Aust. 1995 Jul 3;163(1):50-1. PubMed PMID: 7609693.
Young PB, Kennedy S, Molloy AM, Scott JM, Weir DG, Kennedy DG. Effect of N2O treatment/vitamin B12 deficiency in pigs on tissue concentrations of odd-numbered, branched-chain fatty acids. Int J Vitam Nutr Res.1995;65(4):255-60. PubMed PMID: 8789622.
Louis-Ferdinand RT. Myelotoxic, neurotoxic and reproductive adverse effects of nitrous oxide. Adverse Drug React Toxicol Rev. 1994 Winter;13(4):193-206.Review. PubMed PMID: 7734639.
Flippo TS, Holder WD Jr. Neurologic degeneration associated with nitrous oxide anesthesia in patients with vitamin B12 deficiency. Arch Surg. 1993 Dec;128(12):1391-5. Review. PubMed PMID: 8250714.
Carmel R, Rabinowitz AP, Mazumder A. Metabolic evidence of cobalamin deficiency in bone marrow cells harvested for transplantation from donors given nitrous oxide. Eur J Haematol. 1993 Apr;50(4):228-33. PubMed PMID: 8500605.
Koblin DD, Tomerson BW, Waldman FM, Lampe GH, Wauk LZ, Eger EI 2nd. Effect of nitrous oxide on folate and vitamin B12 metabolism in patients. Anesth Analg. 1990 Dec;71(6):610-7. PubMed PMID: 2240633.
Koblin DD, Tomerson BW, Waldman FM. Disruption of folate and vitamin B12 metabolism in aged rats following exposure to nitrous oxide. Anesthesiology. 1990 Sep;73(3):506-12. PubMed PMID: 2393136.
van Achterbergh SM, Vorster BJ, Heyns AD. The effect of sepsis and short-term exposure to nitrous oxide on the bone marrow and the metabolism of vitamin B12 and folate. S Afr Med J. 1990 Sep 1;78(5):260-3. PubMed PMID: 2392722.
van der Westhuyzen J, Davis RE, Icke GC, Metz J. Tissue folates in fruit bats (Rousettus aegyptiacus) with nitrous oxide-induced vitamin B12 deficiency and neurological impairment. Br J Nutr. 1987 Nov;58(3):485-91. PubMed PMID:3120768.
Van de List C, Combs M, Schilling RF. Nitrous oxide and vitamin B12 deficiency interact adversely on rat growth. J Lab Clin Med. 1986 Oct;108(4):346-8. PubMed PMID: 3760674.
Koblin DD, Biebuyck JF. Is nitrous oxide a dangerous anesthetic for vitamin B12-deficient subjects? JAMA. 1986 Aug 8;256(6):716. PubMed PMID: 3723770.
Schilling RF. Is nitrous oxide a dangerous anesthetic for vitamin B12-deficient subjects? JAMA. 1986 Mar 28;255(12):1605-6. PubMed PMID: 3951096.
McLoughlin JL, Cantrill RC. Nitrous oxide induced vitamin B12 deficiency: measurement of methylation reactions in the fruit bat (Rousettus aegyptiacus).
Int J Biochem. 1986;18(2):199-202. PubMed PMID: 3949064.
Wilson SD, Horne DW. Effect of nitrous oxide inactivation of vitamin B12 on the levels of folate coenzymes in rat bone marrow, kidney, brain, and liver. Arch Biochem Biophys. 1986 Jan;244(1):248-53. PubMed PMID: 3947060.
van Tonder SV, Ruck A, van der Westhuyzen J, Fernandes-Costa F, Metz J. Dissociation of methionine synthetase (EC 2.1.1.13) activity and impairment of
DNA synthesis in fruit bats (Rousettus aegyptiacus) with nitrous oxide-induced vitamin B12 deficiency. Br J Nutr. 1986 Jan;55(1):187-92. PubMed PMID: 3663573.
van der Westhuyzen J, van Tonder SV, Gibson JE, Kilroe-Smith TA, Metz J.Plasma amino acids and tissue methionine levels in fruit bats (Rousettus aegyptiacus) with nitrous oxide-induced vitamin B12 deficiency. Br J Nutr. 1985 May;53(3):657-62. PubMed PMID: 4063293.
O'Leary PW, Combs MJ, Schilling RF. Synergistic deleterious effects of nitrous oxide exposure and vitamin B12 deficiency. J Lab Clin Med. 1985 Apr;105(4):428-31. PubMed PMID: 3981056.
van der Westhuyzen J, Metz J. Betaine delays the onset of neurological impairment in nitrous oxide-induced vitamin B-12 deficiency in fruit bats. J Nutr. 1984 Jun;114(6):1106-11. PubMed PMID: 6726473.
van der Westhuyzen J, Fernandes-Costa F, Metz J. Cobalamin inactivation by nitrous oxide produces severe neurological impairment in fruit bats : protection by methionine and aggravation by folates. Life Sci. 1982 Nov 1;31(18):2001-10. PubMed PMID: 7176808.
Lumb M, Perry J, Deacon R, Chanarin I. Urinary folate loss following inactivation of vitamin B12 by nitrous oxide in rats. Br J Haematol. 1982 Jun;51(2):235-42. PubMed PMID: 7082582.
Kondo H, Osborne ML, Kolhouse JF, Binder MJ, Podell ER, Utley CS, Abrams RS, Allen RH. Nitrous oxide has multiple deleterious effects on cobalamin metabolism and causes decreases in activities of both mammalian cobalamin-dependent enzymes in rats. J Clin Invest. 1981 May;67(5):1270-83. PubMed PMID: 6112240; PubMed Central PMCID: PMC370693.
Steinberg SE, Campbell C, Hillman RS. The effect of nitrous oxide-induced vitamin B12 deficiency on in vivo folate metabolism. Biochem Biophys Res Commun.
1981 Feb 27;98(4):983-9. PubMed PMID: 6164371.
McKenna B, Weir DG, Scott JM. The induction of functional vitamin B-12 deficiency in rats by exposure to nitrous oxide. Biochim Biophys Acta. 1980 Mar 20;628(3):314-21. PubMed PMID: 7370297.
Lumb M, Deacon R, Perry J, Chanarin I, Minty B, Halsey MJ, Nunn JF. The effect of nitrous oxide inactivation of vitamin B12 on rat hepatic folate.Implications for the methylfolate-trap hypothesis. Biochem J. 1980 Mar 15;186(3):933-6. PubMed PMID: 7396845; PubMed Central PMCID: PMC1161731.
Adornato BT. Nitrous oxide and vitamin B12. Lancet. 1978 Dec 16;2(8103):1318. PubMed PMID: 82831.
Deacon R, Lumb M, Perry J, Chanarin I, Minty B, Halsey MJ, Nunn JF. Selective inactivation of vitamin B12 in rats by nitrous oxide. Lancet. 1978 Nov
11;2(8098):1023-4. PubMed PMID: 82036.
Amess JA, Burman JF, Rees GM, Nancekievill DG, Mollin DL. Megaloblastic haemopoiesis in patients receiving nitrous oxide. Lancet. 1978 Aug12;2(8085):339-42. PubMed PMID: 79709.
Selzer, RR, Rosenblatt, DS, Laxova, R, Hogan, K. Adverse effect of nitrous oxide in a child with 5,10-methylenetetrahydrofolate reductase deficiency. New England Journal of Medicine, July 2003; 349: 45–50.
Kalikiri, PC, Sachan Gajraj Singh Sachan, R. Nitrous oxide induced elevation of plasma homocysteine and methylmalonic acid levels and their clinical implications. The Internet Journal of Anesthesiology, 2004; Vol. 8 (2).
Baum, VC. When nitrous oxide is no laughing matter: Nitrous oxide and pediatric anesthesia. Paediatric Anaesthesia, Sept. 2007; 17(9):824-30. https://www.apsf.org/wp-content/uploads/presentations/2018-stoelting/Nitrous-Oxide-Vitamin-B12-Destruction-and-Myeloneuropathy-Kirk-Hogan.pdf https://www.haveyoursay.nsw.gov.au/nitrous-oxide-reform
Copyright © 2014 B12 Oils. All Rights Reserved.
Reproduction in whole or in part in any form or medium without express written
permission is prohibited